2014
1
Autores:
Victoria García V1, Luis Guillermo Echavarría R.2, Ricardo Ardila C.3, Jorge Gutiérrez M.4
Instituciones:
1Departamento de Ginecología y Obstetricia-Medicina Crítica y Cuidado Intensivo, 2Departamento de Ginecología y Obstetricia, 3Departamento de Medicina Interna, Epidemiología, 4Departamento de Medicina Materno Fetal. Clínica Universitaria Bolivariana. Medellín, Colombia.
Imágen 1:
Imágen 2:
Imágen 3:
Tipo de documento:
Trabajos OriginalesHALLAZGOS CLÍNICOS Y DE LABORATORIO QUE SUGIEREN TEMPRANAMENTE EL SÍNDROME DE HELLP EN PACIENTES CON PREECLAMPSIA SEVERA
Contenido del documento:
RESUMEN
Objetivo: Determinar la utilidad de las pruebas de laboratorio y clínicas que se alteran de forma precoz para el diagnóstico del síndrome de HELLP en pacientes con preeclampsia severa.
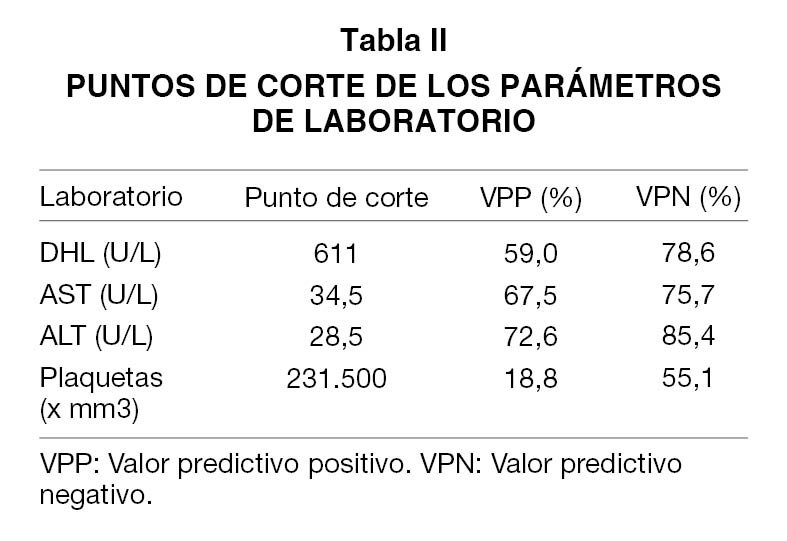
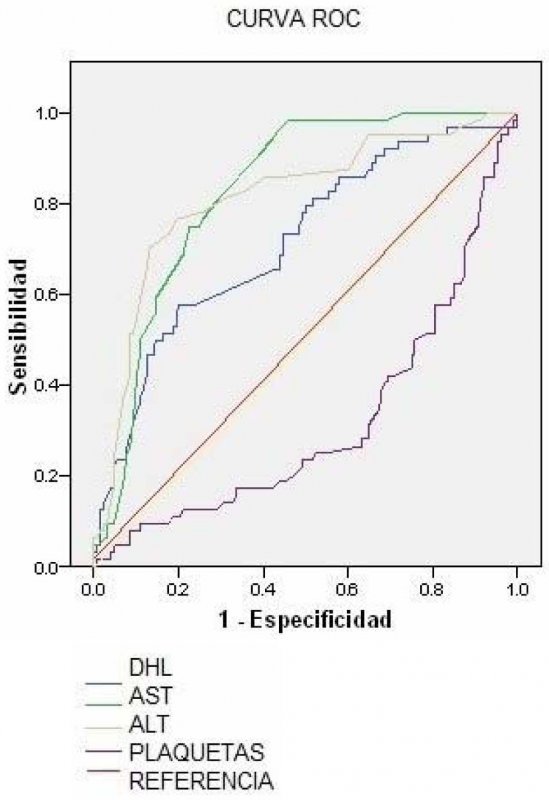
Métodos: Estudio observacional retrospectivo, de utilidad de prueba diagnóstica, basado en una cohorte clínica que incluyó mujeres embarazadas con diagnóstico de preeclampsia severa ingresadas entre el 4 de mayo del 2005 al 7 mayo del 2008 en la Clínica Universitaria Bolivariana (CUB). Se realizó comparación entre los dos grupos (HELLP y no HELLP) en las variables estudiadas. Se calculo la sensibilidad, la especificidad, los valores predictivos y las LR (+ y -), y sus IC al 95 %, comparando cada una de las variables clínicas, con la prueba oro: diagnóstico final de HELLP. Se realizaron curvas ROC para las pruebas cuantitativas en la hospitalización para identificar cual es el parámetro de laboratorio que mejor determina el desarrollo del síndrome de HELLP.
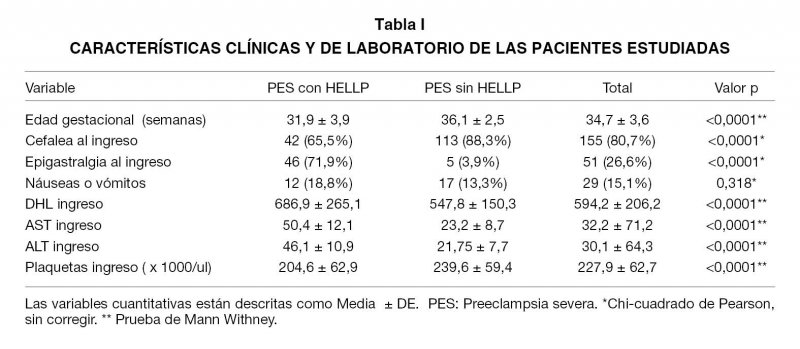
Resultados: El dolor en epigastrio fue el factor clínico predictor más importante en los pacientes con pre eclampsia severa que desarrollaron HELLP con un valor de p<0,0001; de las pruebas de laboratorio realizadas al ingreso, las transaminasas fueron significativamente mayores en las pacientes con preclampsia severa que desarrollaron síndrome de HELLP. Conclusión: En las pacientes con diagnóstico de preeclampsia severa la presencia de epigastralgia y/o transaminasas elevadas son hallazgos que sugieren tempranamente el desarrollo de síndrome de HELLP.
PALABRAS CLAVE: Preeclampsia, síndrome de HELLP, factores predictores
SUMMARY
Objectives: The aim of this study was to determine the usefulness of precociously altered clinical and laboratory tests for the diagnosis of HELLP in patients with severe preeclampsia.
Methods: An observational study was performed, utility of diagnostic tests, based on a clinical cohort which included pregnant women diagnosed with severe preeclampsia admitted between May 4, 2005 and May 7, 2008 in the Clinica Universitaria Bolivariana was conducted. Comparison was made between the two groups (HELLP and non HELLP) on the assessed variables. Sensitivity, specificity, predictive values and the LR (+ and -) and their 95% CI were calculated, comparing each of the clinical variables with the golden standard test: final diagnosis of HELLP. ROC curves were performed for the laboratory quantitative tests during hospitalization to identify which is the laboratory parameter that best determines the development of HELLP syndrome.
Results: Epigastrium pain was the most important predictive factor in clinical patients with severe preeclampsia who developed HELLP with a value of p<0.0001. The values of laboratory tests and transaminases conducted at admission were significantly higher in patients with severe preeclampsia who developed HELLP syndrome.
Conclusion: This study found that in patients diagnosed with severe preeclampsia, the presence of epigastric pain and / or transaminases are findings suggest the early development of HELLP syndrome, for that reason changes of liver tests and the presence of epigastric pain should be actively tracked in this group of patients.
KEY WORDS: Preeclampsia, HELLP syndrome, predictors
PACIENTES Y MÉTODOS
RESULTADOS
CONCLUSIÓN
BIBLIOGRAFÍA
1. Haram K, Svendsen E, Abildgaard U. The HELLP syndrome: Clinical issues and management. A review. BMC Pregnancy Childbirth 2009;9:8-23.
2. Magee LA, Helewa M, Moutquin JM, von Dadelszen P. Diagnosis, evaluation, and management of the hypertensive disorders of pregnancy. J Obstet Gynaecol Can 2008;30(3 suppl):S1-48.
3. Steegers EA, von Dadelszen P, Duvekot JJ, Pijnenborg R. Pre-eclampsia. Lancet 2010;376(9741):631-44.
4. Joshi D, James A, Quaglia A, Westbrook RH, Heneghan MA. Liver disease in pregnancy. Lancet 2010;375(9741):594-605.
5. Guzel AL, Kuyumcuoglu U, Celik Y. Are maternal and fetal parameters related to perinatal mortality in HELLP syndrome? Arch Gynecol Obstet 2011;283:1227-32.
6. Connealy BD, Carreno CA, Kase BA, Hart LA, Blackwell SC, Sibai BM. A history of prior preeclampsia as a risk factor for preterm birth. Am J Perinatol 2013; [Epub ahead of print].
7. Martin JN Jr, Blake PG, Lowry SL, Perry KG Jr, Files JC, Morrison JC. Pregnancy complicated by preeclampsia-eclampsia with the syndrome of hemolysis, elevated liver enzymes and low platelet count: how rapid is postpartum recovery? Obstet Gynecol 1990;76:737-41.
8. Martin JN Jr, Blake PG, Perry KG, McCaul JF, Hess LW, Martin RW. The natural history of HELLP syndrome: patterns of disease progression and regression. Am J Obstet Gynecol 1991;164:1500-13.
9. Isler CM, Martin JN Jr. Preeclampsia: pathophysiology and practice considerations for the consulting nephrologist. Semin Nephrol 2002;22:54-64
10. Vigil-De Gracia P, Ortega-Paz L. Pre-eclampsia/eclampsia and hepatic rupture. Int J Gynecol Obstet 2012;118:186-9.
11. Weinstein L. Preeclampsia/eclampsia with hemolysis, elevated liver enzymes and thrombocytopenia. Obstet Gynecol 1985;66:657-60.
12. Sibai BM. Diagnosis, Controversies, and Management of the Syndrome of hemolysis, elevated liver enzymes, and low platelets count. Obstet Gynacol 2004;103:981-92.
13. Martin JN Jr, May WL, Magann EF, Terrone DA, Rinehart BK, Blake PG. Early risk assessment of severe preeclampsia: admission battery of symptoms and laboratory tests to predict likelihood of subsequent significant maternal morbidity. Am J Obstet Gynecol 1999;180:1407-14.
14. Carpani G, Bozzo M, Ferrazzi E, D’Amato B, Pizzotti D, Radaelli T, Moroni G, Pardi G. The evaluation of maternal parameters at diagnosis may predict HELLP syndrome severity. J Matern Fetal Neonatal Med 2003;13:147-51.
15. Von Dadelszen P, Payne B, Li J, Ansermino JM, Broughton Pipkin F, Cote AM, et al; PIERS Study Group. Prediction of adverse maternal outcomes in pre-eclampsia: development and validation of the fullPIERS model. Lancet 2011;377(9761):219-27.
16. Baxter JK, Weinstein L. HELLP syndrome: The state of art. Obstet Gynecol Surv 2004;59:838-45.
17. Nisell H, Palm K, Wolff K. Prediction of maternal and fetal complications in preeclampsia. Acta Obstet Gynecol Scand 2000;79:19-23.
18. Ganzevoort W, Rep A, de Vries J, Bonsel GJ, Wolf H. Prediction of maternal complications and adverse infant outcome at admission for temporizing management of early-onset severe hypertensive disorders of pregnancy. Am J Obstet Gynecol 2006;195:495-503.